
Carnival Crazy: Another aspect of Canarian distinctiveness.
Maybe not crazy, but definitely divergent from the rest of Spain in mental health.

It’s Carnival time here in the Canary Islands.

I have to admit that the controlled craziness of Carnival has a certain appeal. And I’m not just saying it because a guy in a black widow costume called me handsome. There’s something to be said for the rule-breaking spirit of Carnival and the blowing off of steam in massive public celebrations.
On the other hand, twice in the last month I’ve been screamed at in public for no particular reason. Canarians have a deserved reputation for being very talkative, and after a couple of years living in Andalusia I’ve grown used to strangers striking up conversations with me, but I could do without the shouting.
After these events, and a few others that would take too long to recount1, I decided to take a look at the mental health statistics for the Canary Islands. I didn’t believe Carnival madness was really an expression of the revellers’ mental health, but the shouting did make me contemplate the possibility of an underlying cause.
Well, according to the 2023 Spanish National health system annual report (as reported by the Spanish press), the mental health of Canarians is the worse among all Spanish regions2:
The [Spanish] age-adjusted prevalence [of behavioral and mental disorders] was 331 cases/1,000, which is 4.7% higher than in 2019.
By region, the highest figures were in the Canary Islands (518.5); Valencian Community (466.8) and Murcia (424.3), while Castilla-La Mancha (103.4); Extremadura (132.9); Andalusia (135.4) and the Basque Country (299.4) did not reach the national average.
Notice that the regions of Andalusia, Extremadura and Castilla-La Mancha show substantially lower rates of behavioral and mental disorders than the Spanish average. This is particularly interesting because these three regions form what is commonly understood as Southern Spain3, and the Canary Islands are usually grouped together with them, due to a similar culture and the Andalusian origin of a large share of the islands’ early colonists. And yet, remarkably, the Canaries differ widely from Southern Spain in terms of mental health.
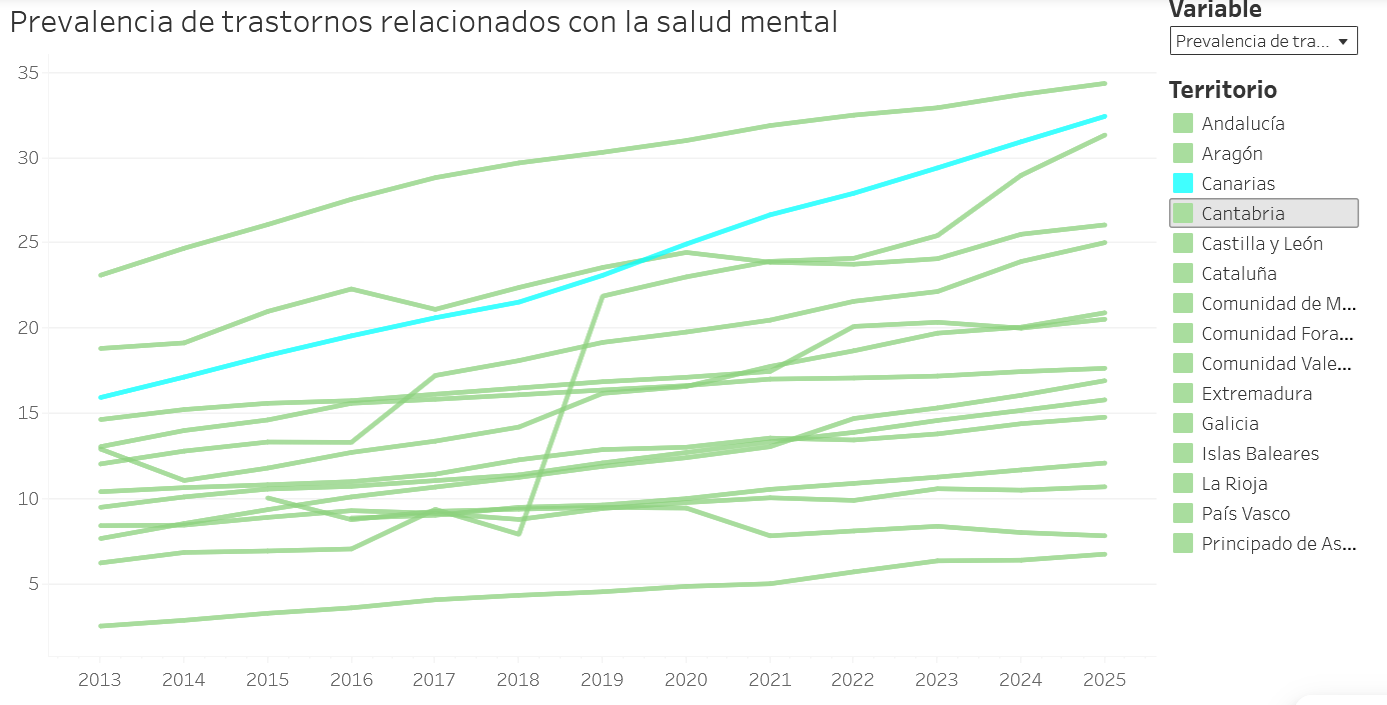
This high rate of mental disorders is not a recent phenomenon. As you can see in the following chart, this has been the case for more than a decade - though notice that the Valencian Community shows a higher rate in the chart4.
And this pattern aligns with other mental health indicators, such as the suicide rate per 100,000 people. While the Canary Islands do not display the highest raw suicide rate in the next chart, this is likely a result of not adjusting by age structure, as Asturias (highest) and Galicia (second-highest) have the oldest populations in Spain.
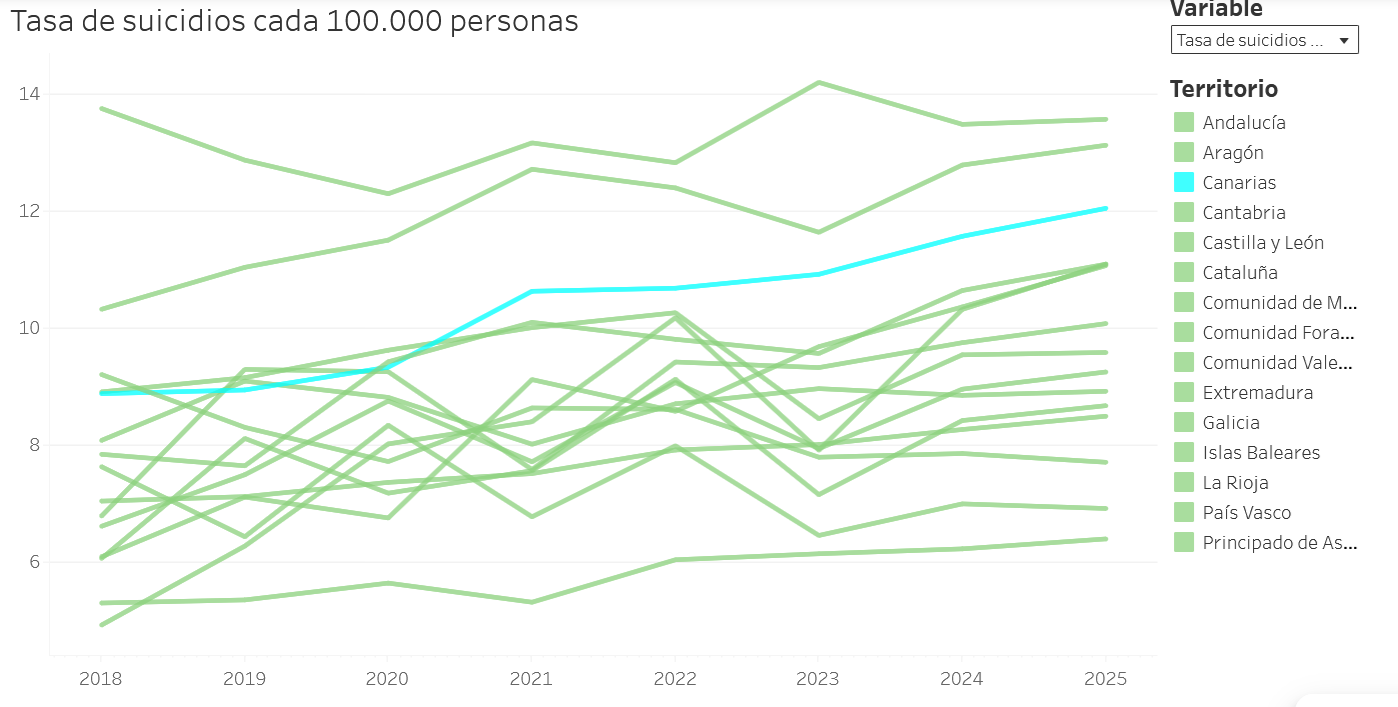
In contrast to Asturias and Galicia, the Canaries have a relatively young population structure, which lowers its raw suicide rate compared to older regions since suicide rates usually peak in older cohorts. Using a crude age adjustment5, I confirmed that age-adjusted male suicide rates in the Canary Islands were roughly the same as those in Asturias and Galicia in the years before 2020 (prior to Covid-19), and that a substantial gap exists between the archipelago’s high rate and the (average looking) rates seen in the other Southern Spanish regions.

Furthermore, a 2017 Spanish health ministry’s breakdown of mental health diagnoses6 shows that rates of mental disorders among older people are not exceptionally high in the archipelago7. Disorders affecting the young seem to be more prevalent than the Spanish average8, while those not specific to young or old exhibit exceptionally high rates: phobias, schizophrenia, other organic psychosis9, etc. The only exception in this last category is affective psychosis, with a rate roughly half the national average10.
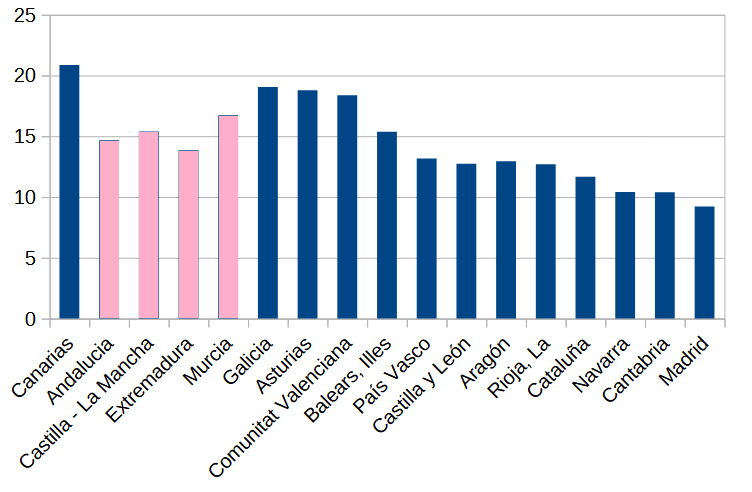
Lastly, we can examine the rates of accidental poisoning deaths by psychotropic drugs and drugs of abuse, a specific cause of death recorded by Spain’s National Institute of Statistics (INE). Although this indicator may not track mental health as closely as the others, the Canary Islands again show up among the highest ranked regions.
What about Latin America?
I believe the previous figures clearly establish that Canarian mental health indicators diverge from the rest of Spain, but I must acknowledge that I have no evidence this pattern has existed for longer than the last couple of decades. Asking whether this also holds in Hispanic Latin America among populations of Canarian descent compared to those from other Spanish regions implicitly assumes that this is not a recent phenomenon, but a long-lasting one that is endogenous to the Canarian population. Yet, I can’t find any way to measure the mental health of Canarians and other Spaniards in the 17th or 18th century. While I examine Latin American mental health indicators in the following paragraphs, please keep in mind that if Latin American regions with heavy Canarian settlement have worse mental health than other regions there’s a substantial probability this is just a coincidence.
Nevertheless, it might be worthwhile to check whether this mental health pattern holds on the other side of the Atlantic, at least to test the hypothesis that Canarians’ poor mental health is a long-lasting phenomenon which traveled across the ocean along with Canarian culture.
Let’s start with suicide rates. The countries we want to focus on are the ones that received the largest Canarian migration flows and therefore have the highest share of Canarian ancestry (what I call Canari America):
[Canarians] played a significant role in shaping the contemporary societies of a few countries: Cuba, the Dominican Republic, Puerto Rico, Uruguay, and Venezuela11.
Well, Uruguay, Cuba and and Venezuela had the three highest suicide rates in Latin America in 2021, with 24.8, 13.8 and 8.6 suicides per 100,000 people respectively.

Those suicide rates tentatively suggests the pattern holds, but let’s continue by looking at other death rates related to mental health. For this I’ll rely on data from Our World in Data, which compiles death rates by country based on World Health Organization (WHO) statistics. These are the rates published by Our World in Data, along with the ranking of our countries of interest within Latin America12:
Alcohol and drug use disorders (2021): Cuba (third), Uruguay (fifth).
Mental health and substance use disorders deaths: Cuba (third), Uruguay (fifth).
Drug use disorder death rate: Uruguay (fifth).
Some of these rates clearly overlap each other, so don’t take them as three separate pieces of evidence, but rather as one additional piece of evidence suggesting poor mental health in the countries of Canari America, even if not very strongly (notice none of the countries ranks first or second).

Also, even though a country’s overall mental health is just one of several factors influencing the number of psychiatrists in that country, I should point out that Uruguay has the highest ratio of psychiatrists per 100,000 people, and Cuba the third-highest in Latin America, according to Our World in Data13.
Taken together, these figures imply that the Canarian mental health pattern may hold in Latin America, at least in some countries and at least recently. In the case of Venezuela though, only its high suicide rate suggests poor mental health, and I couldn’t find other recent data that would support this hypothesis. But I did find one interesting piece of not so recent data.
The 1941 Venezuelan census
People in 1941 were not as politically correct as they are today. They had no compunctions about calling the intellectually disabled “idiots”, and those suffering from mental health disorders “crazies”. So it’s not surprising that the designers of the 1941 Venezuelan census thought it was a good idea to record the number of people suffering from physical and mental defects, including those classified as idiots and crazies, allowing us to examine the rates and figures of people classified as such by census takers in each Venezuelan state at that time.
You might recall that I’ve written before about the cultural differences between Venezuelan regions:

.svg){kind=link}
And how Venezuela’s Caribbean coastal region seems to be more culturally similar to the Canary Islands, while its Andean region differs from both.
Well, the 1941 census allows us to test whether cultural differences between these two regions also extend to mental health differences by looking at the rates of crazies per 100,000 people in each Venezuelan state14.
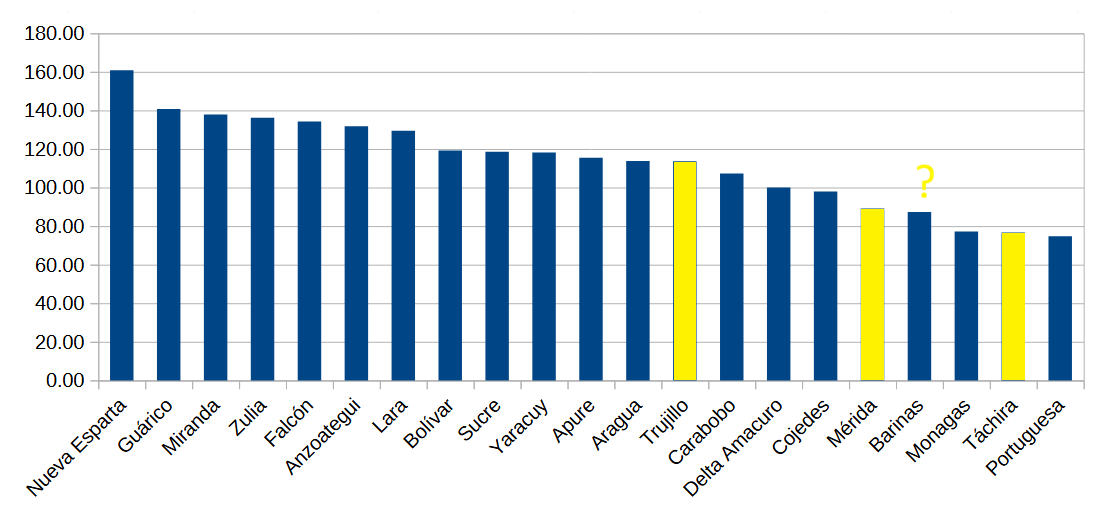
The three Andean region states (Mérida, Táchira and Trujillo) show low rates of “crazies”, but not exceptionally low. And, of course, it’s also possible that census takers did not evaluate mental health in a uniform manner across Venezuelan states.
You’ll also notice that I marked Barinas state with a question mark in the above chart. Although it’s not geographically part of the Andes, Barinas borders all three Andean states and, as shown in the election maps from my previous Venezuela post15, it can be grouped with the Andean states when it comes to political leanings (UPDATE: In fact, more than 10% of its 1941 population had been born in an Andean state).
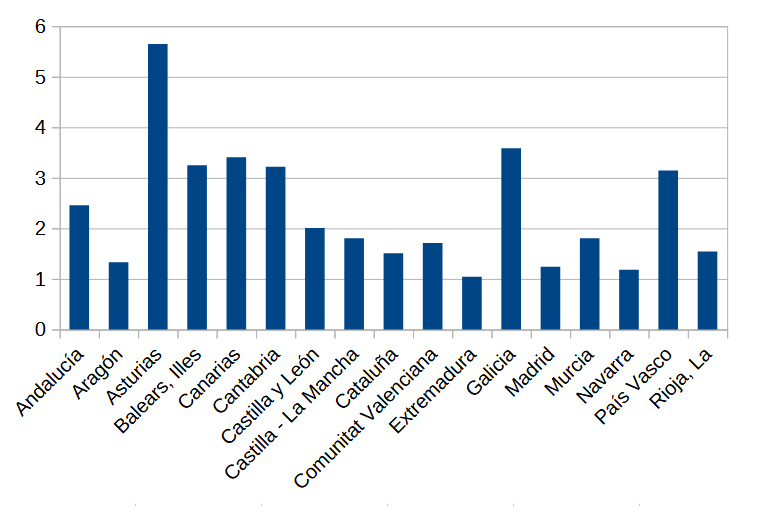
To account for the possibility that our politically incorrect census takers applied different thresholds when classifying mental disabilities across Venezuelan states, let’s examine the ratio of crazies to all mental disabilities (crazies plus idiots)16.
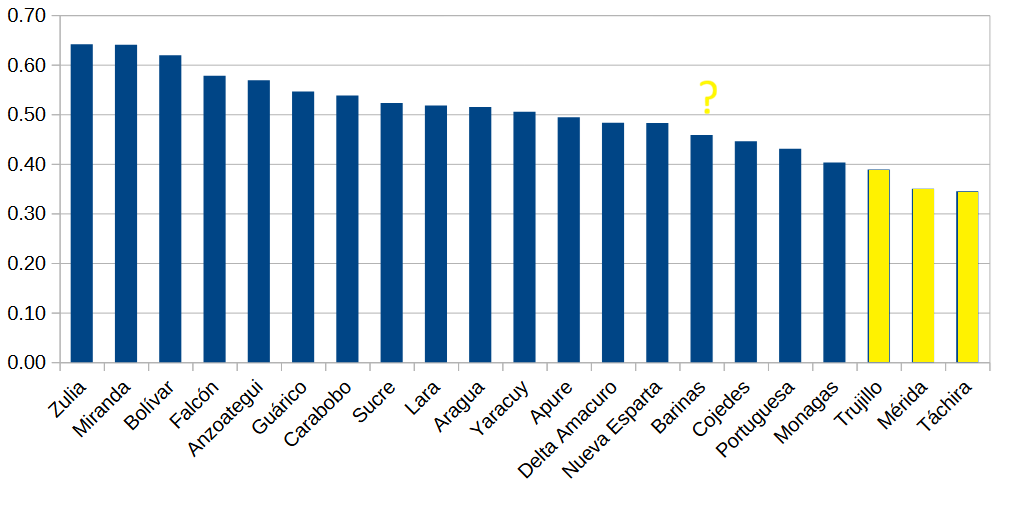
That looks like stronger evidence that Andean Venezuelans suffer from lower rates of mental health disorders than other (more Canarian) Venezuelans17. Or at the very least, that craziness was understood in a different way in one cultural region than in the other. This is not definitive proof that the Canarian mental health pattern also holds in Latin America, but it’s suggestive enough that the possibility should not be dismissed.
So to sum up, the Canary Islands do not indisputably have the poorest mental health in Spain, but they clearly rank among the regions with the worst mental health indicators. Notice, though, that other regions with similarly poor mental health indicators (Murcia, Valencia) contributed little to the Spanish settlement of the Americas, so perhaps the Canary Islands have the worst mental health profile among the regions that made a substantial contribution to the peopling of Latin America.
Secondly, there is at least some evidence - though not conclusive - that countries and regions of Latin American which experienced heavy Canarian settlement show worse mental health indicators than the rest of Latin America. This is hardly definitive, but it is another factor worth considering when trying to explain why Canari America diverges from the rest of Latin America.
Ok, one. A few minutes ago, while I was waiting for the tram to arrive and scrolling on my phone (I know, I know), I noticed out of the corner of my eye that people were clustering close to me. I looked up and saw a homeless-looking guy shouting (though not loud enough for me to notice until that moment) at some of the waiting passengers on the platform: “I won’t tell you anything! I won’t tell you anything!”. The passengers close to him moved to create a four or five meter “safety” zone around the shouting homeless guy (thus the bunching up), who just kept shouting (“someone could die!”). This isn’t especially dramatic, and of course doesn’t have to reflect the mental health of the population at large, but it is a situation that I’ve seen happen several times already in the few weeks I’ve been in the Canaries.
Together with Murcia, though.
This is likely because the plotted rates have not been adjusted by age.
I based my age-adjustment on the Spanish INE’s figures, quoted by Ruiz-Vega, A., Montero-Alonso, M.A. and Luna, J. (2025).
Source is BDCAP 2017 database. The data can be downloaded from here (“Tablas de datos. Salud mental“ link).
The Canary Islands has the fourth-highest incidence of dementia, but has the lowest rate of memory disorders among the 75 and older population.
The rate of learning disorders among those aged 25 years and younger is higher than the national average. Enuresis rates are very low; hyperkinetic disorders rank third-highest in Spain; stuttering rate is slightly above average; and anorexia among those aged 15-39 is also slightly above average.
The rate of Other organic psychosis in the Canary Islands looks suspiciously high; ten times higher than the rate in the second-highest region.
The incidence rates for all other disorders are: other organic psychoses rank highest, phobias second-highest, unspecified psychosis third-highest, schizophrenia second, somatization disorders second, personality disorders third, anxiety disorders third, obsessive compulsive disorder third, general adaptation reaction fourth, and sleep disorders fifth.
I omitted deaths for very specific substances: opioids, amphetamines, cocaine.
Psychiatrists per 100,000 people, Our World in Data. Based on data from Unicef (System Strength, Human resource levels).
I excluded the Distrito Federal due to its extremely high crazies ratio (269.7), which I assume is connected to it being the country’s capital (highly urbanized, and maybe high concentration of mental asylums).
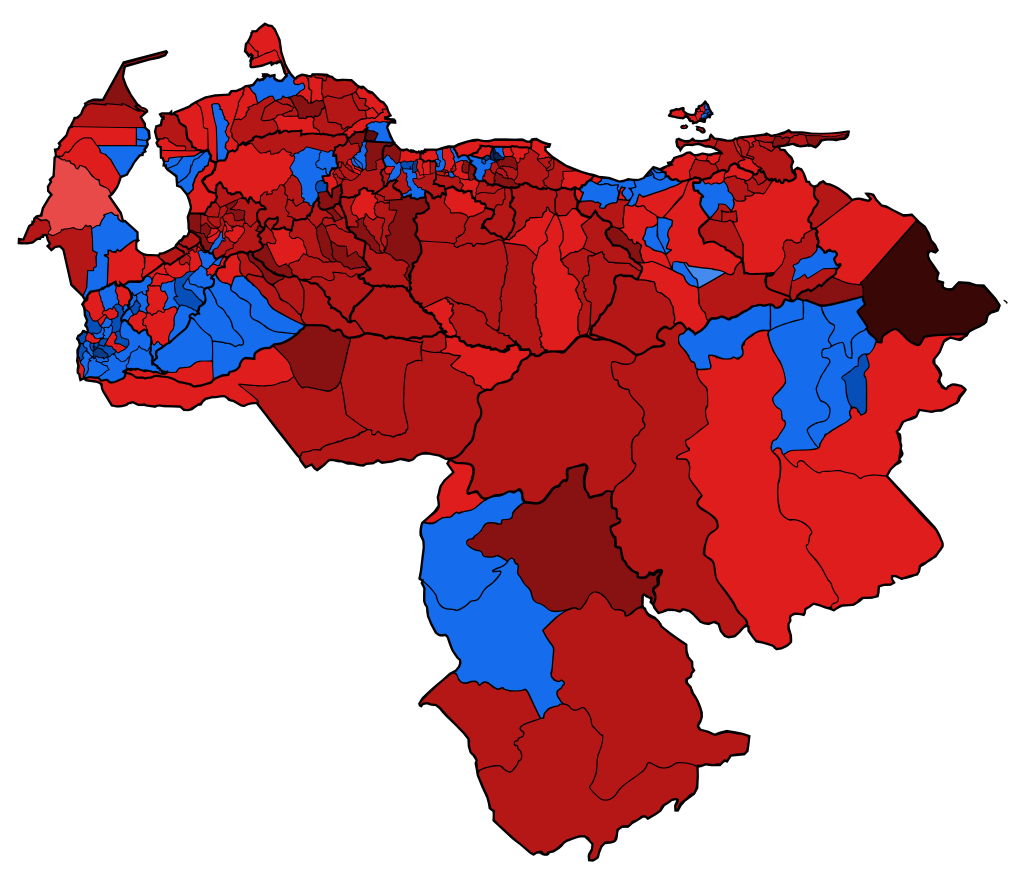
Here’s one of those maps (2013 presidential election), followed by a Venezuela map showing the location of Barinas, in case you don’t want to click on that link:

Other disability categories recorded in the census are: Blind, limp, hunchback, one-armed, deafblind, and other defects.
Additionally, I calculated an alternative crazies ratio that includes the Other defects category in the denominator, although it’s not explicitly stated whether this category includes mental disorders. This change’s only effect on the state ranking is swapping the positions of Trujillo and Monagas.